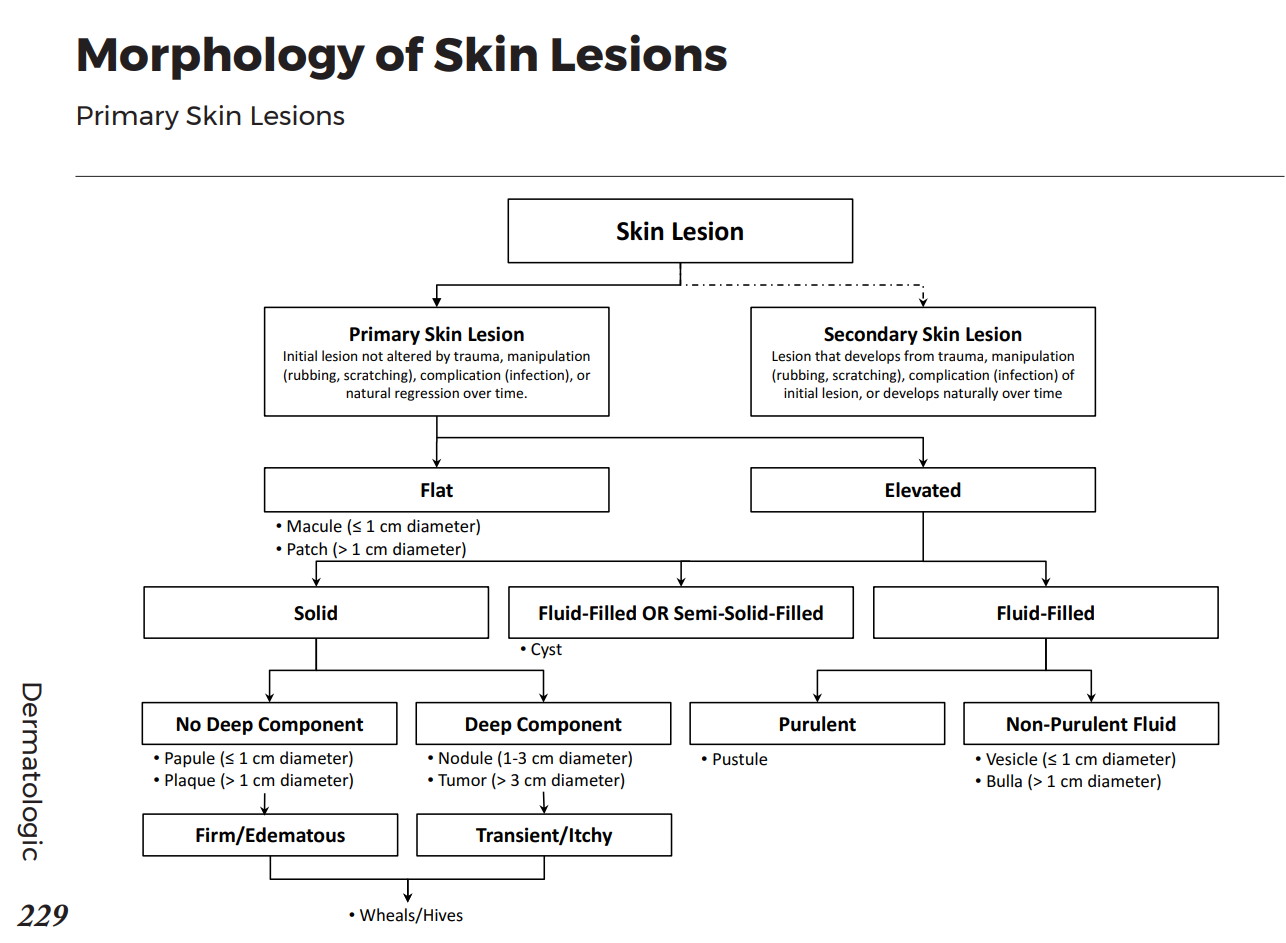
Describing lesions
Primary lesion: de-novo un-altered lesion Secondary lesion: evolution of 1' lesion
Basic lesion descriptors
| Profile | <1cm diameter | >1cm diameter |
|---|---|---|
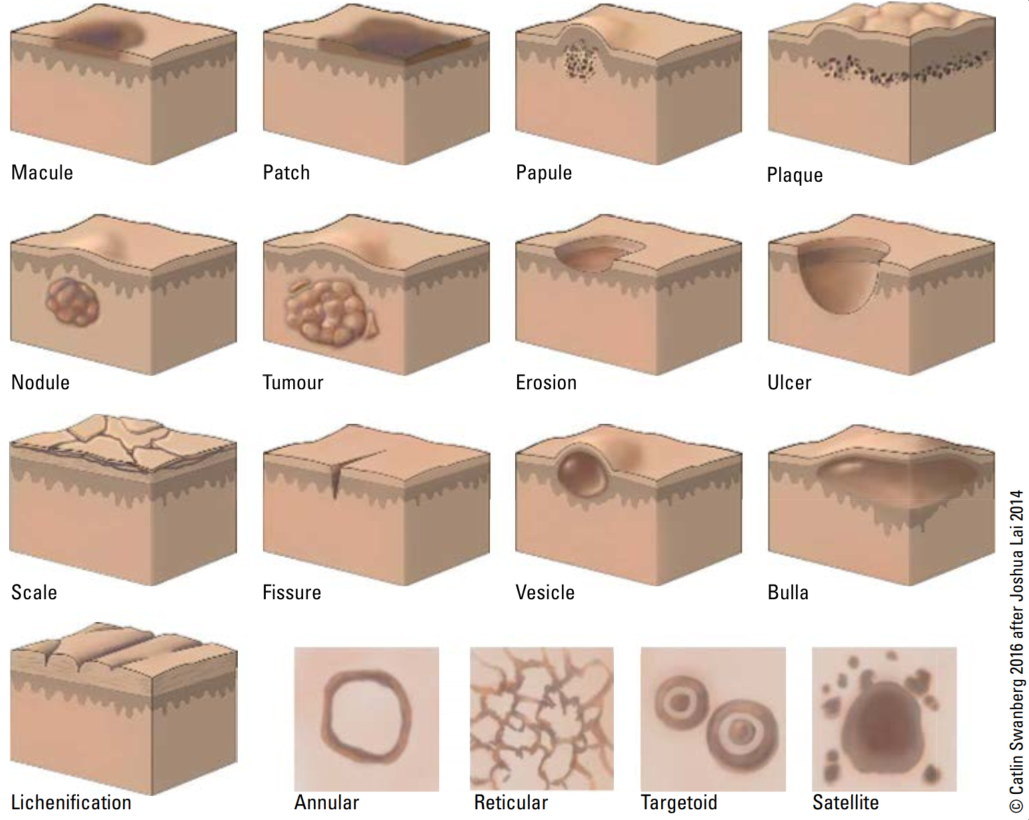
| Flat | Macule | Patch |
| Raised superficial | Papule | Plaque |
| Deep palpable | Nodule | Tumor |
| Fluid filled | Vesicle | Bulla |
Other lesion nomenclature
| Excoriation: | Traumatized or abraded skin, usually due to scratching or rubbing. |
|---|---|
| Scale: | Flakes of keratin that can be fine or coarse; loose or adherent. Example: Dandruff, seborrheic dermatitis |
| Erosion: | Superficial open wound involving only epidermis or mucosa. Does not extend into the underlying dermis, so healing occurs without scar formation. |
| Ulcer: | Deep open wound extending into the dermis or subcutaneous tissue. May lead to scar formation. Example: Diabetic foot ulcer, Canker sore |
| Crust: | Dried fluid (serum, blood, or purulent exudate) originating from a lesion (e.g. impetigo) |
| Eschar: | A scab or dry crust that results from trauma, infection, or excoriating skin disease. It is necrotic tissue. |
| Lichenification: | thickening of the skin and accentuation of normal skin markings (e.g. chronic atopic dermatitis) usually from chronic rubbing/itching |
| Fissure: | Linear slit-like cleavage of the skin |

|

|

|

|
|

|

|
| Cyst | an internally epithelial, endothelial, or membrane lined structure containing semi-solid material or fluid |
|---|---|
| Pustule | an elevated lesion containing pus |
| Scar | replacement fibrosis of dermis and subcutaneous tissue (hypertrophic or atrophic) |
| Wheal/hives | a special form of papule or plaque that is transient (<24 h) and blanchable, often with a halo and central clearing, formed by edema in the dermis (e.g. urticaria) |
| Comedone | a special collection of sebum and keratin (whiteheads (open) / blackheads (closed) |
| Petechiae | pinpoint extravasation of blood into dermis resulting in hemorrhagic lesions; nonblanchable, <3 mm in size, usually flat |
| Purpura | larger than petechia, 3 mm-1 cm in size. Like tiny bruises, red/purple macules or papules from capillary hemorrhages under skin. DO NOT blanch with pressure. May be raised. Example: Thrombocytopenic purpura |
| Ecchymosis | larger than purpura, >1 cm in size (i.e. a “bruise”) |
| Telangiectasia | dilated superficial blood vessels; blanchable, reticulated, and of small calibre, can be associated with benign or malignant entities |

|

|

|

|

|

|

|

|
Pattern nomenclature
| Maculopapular: | rash has both macules and papules |
|---|---|
| Annular: | Ring-like. |
| Arcuate: | Curved, resembling an arc(s). |
| Polycyclic: | Multiple curves, like the edge of a cloud. |
| Reticulate/Reticular: | Mottled. |
| Zosteriform/dermatomal: | distributed along dermatomal lines, like Shingles. |
| morbilliform: | literally means “measles-like”, an eruption composed of macules and papules with truncal predominance |
| satellite: | small lesions scattered around the periphery of a larger lesion (e.g. candida diaper dermatitis) |
| target/targetoid: | concentric ring lesions, like a dartboard (e.g. EM) |
| other descriptive terms: | Grouped, linear, follicular, discrete, clustered, indurated, fluctuant |

|

|

|

|

|

|

|

|
Approach to skin lesions
Lesion History
- Onset
- Location
- Pattern of spread
- Evolution
- Provoking factors (ie heat, cold, sun, exercise, travel, medications, pregnancy, season
- Associated symptoms (ie pain, itch)
Associated symptoms
- Acute: headache, chills, fever, weakness, night sweats
- Chronic: fatigue, weakness, anorexia, weight loss
Other particular things on consult history
- PMHx any skin conditions, chronic diseases, etc; FHx of psoriasis, atopy, melanoma, etc; Social history focus on travel and chemical exposures, home environment, sick contacts; Meds, don't forget OTC
Diagnosis
Often hinges on history and physical exam. Frequently however, biopsy may be done to confirm or establish a diagnosis.
HISTORY PEARL
Remember SCALDA to describe a lesion:- S - Size/Shape/texture
- C - Colour
- A - Arrangement
- L - Lesion type - primary vs secondary
- D - Distribution - ie Symmetrical, dermatomal, follicular, extensor surfaces, intertriginous (between body folds), dependent areas, sun-exposed skin
- A - Always check condition/involvement of mucous membranes, nails, hair, and intertriginous areas
Common treatments
Topical steroids
| Potency | Relative Strength | Generics | Brand | Usage |
|---|---|---|---|---|
| Weak | x1 | hydrocortisone–2.5% (1% and 0.5% available over-the-counter) | Emo cort | Intertriginous areas, children, face, thin skin |
| Moderate | x3 | betamethasone-valerate-0.1%; hydrocortisone 17-valerate-0.2%; desonide; mometasone furoate | Betaderm; Hydroval; Tridesilon; Elocom | Arm, leg, trunk |
| Potent | x6 | amcinonide | Cyclocort | Body |
| Very potent | x9 | betamethasone dipropionate-0.05%; fluocinonide-0.05%; halcinonide | Diprosone; Lindex; Lyderm; Halog | Palms and soles |
| Extreme | x12 | Clobetasol propionate-0.05% (most potent); betamethasone-dipropionate ointment; halobetasol proprionate-0.05% | Dermovate; diprolene; ultravate | Palms and soles |
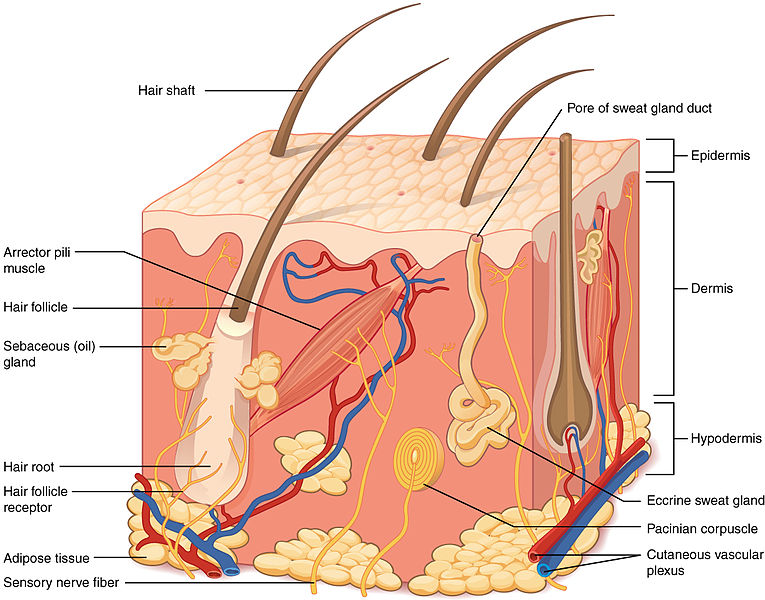
PHSYIOLOGY
Skin functions:
- Protection: continuous recycling and avascularity of epidermis; barrier to UV radiation (melanin), mechanical/chemical insults (sensory/mechanoreceptors), pathogens (immune cells, bactericidal chemicals in sebum, acidic sweat), and dehydration (lipid rich barrier)
- Thermal Regulation: insulation to maintain body temperature in cool environments; dissipation of heat in warm environments via sweat glands and increased blood flow
- Sensation: touch, pain, temperature
- Metabolic: vitamin D synthesis, energy storage of adipose tissue
- Excretion and absorption: Loss of fluid through sweat, carbon dioxide. Small absorption of lipid-soluble materials (ie gases, steroids, KADE, some toxins).
Skin Flora
- Skin microflora is dominated by staphylococci (especially coagulase-negative staphylococci, which are a collection of different organisms), streptococci (B hemolytic, especially), corynebacteria, and propionibacterium.
- Skin near the perineum and rectal region tends to have more enteric organisms present, such as enterobacteriaceae, enterococci, and bacteroides species.
- Keratinocytes and other constituents of skin prevent colonization by other (relatively pathogenic) organisms; when skin is unhealthy, they are prone to colonization by pathogenic organisms (such as S. aureus in patients with psoriasis).
Resources / Image References
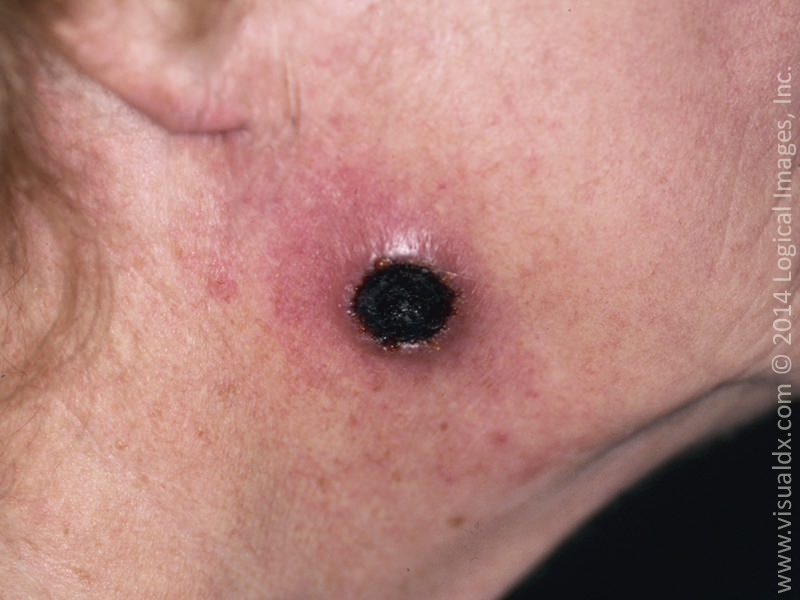
- LearnDerm by visualdx is an amazing resource for fundemental dermatology and has an excellent collection of photos. Click HERE to see more.
- American Family Physician: 1) Generalized Rash DDx 2) Generalized Rash Approach 3) Derm Emergencies 4) Index of other articles
- DermNet NZ is a free wiki with lots of pictures about many conditions. https://dermnetnz.org/
- https://canadiem.org/describing-a-rash/
- Toronto Notes 2020
- American Academy of Dermatology
- UBC's pediatric guide to skin lesions